 加载中…
加载中…Biofilms in Dermatology
标签:
杂谈 |
Biofilms in Dermatology
Aron G. Nusbaum, BS; Robert S. Kirsner, MD, PhD; Carlos A. Charles, MD
Posted: 07/27/2012;
Skin Therapy
Letter.
Abstract
Biofilms are diverse communities of microorganisms embedded within a self-produced matrix of extracellular polymeric substance which are firmly attached to biotic or abiotic surfaces. Approximately 80% of all human infections are associated with biofilms and evidence for their role in an ever-growing number of cutaneous disorders is constantly unfolding. Biofilms present a difficult challenge to clinicians due to their persistent nature, inability to be cultured with standard techniques, and resistance to conventional antimicrobial therapy. Although limited treatment options are presently available, better understanding of the molecular biology of biofilms and their pathogenicity will likely lead to the development of novel anti-biofilm agents for clinical use.
Introduction
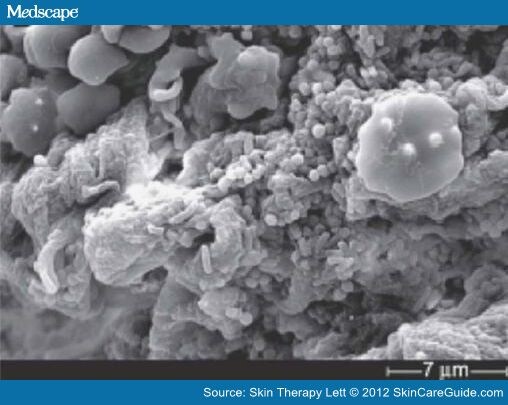
While bacteria have classically been viewed from the perspective of planktonic, free floating pathogens proliferating and exerting their virulence as individual organisms, it is now recognized that microbes also can exist as multicellular consortiums known as biofilms.[1,2] (Figure 1) Several advantages exist for bacteria that live in a biofilm phenotype including structural stability, firm adherence to biotic or abiotic surfaces, increased virulence, and resistance to both antimicrobial therapy and the host immune response. Organisms within biofilms are embedded in a glycocalyx, a self-produced matrix of extracellular polymeric substance (EPS) composed of polysaccharides, proteins, lipids, and extracellular DNA (eDNA). The EPS is considered to be the hallmark of biofilm formation and in addition to facilitating attachment, it also serves a protective function by preventing neutrophilic penetration,[2] masking phagocytic detection of opsonins,[3] and sequestering host antibodies, as well as complement factors.[4] The formation and behavior of the entire biofilm community is directed by signaling molecules that are produced when microorganisms reach a critical number. This phenomenon is termed quorum sensing (QS) and has also been shown to regulate the expression of virulence factors as well as modulate host immunity.[5]
{kind=link}
Figure 1.Scanning electron micrograph demonstrating the presence of mixed species biofilm in a chronic wound. Both cocci and bacilli are seen embedded in an amorphous matrix characteristic of biofilm formation.Figure from James GA, Swogger E, Wolcott R, et al. Biofilms in chronic wounds. Wound Repair Regen. 2008 Jan-Feb;16(1):page 42, Figure 1D. Reprinted with permission from John Wiley and Sons.
Biofilms have been associated with approximately 80% of all human infections, yet their detection is extremely difficult with the use of routine culture techniques.[6] New methods to detect biofilm-associated organisms are under development. For example, denaturating gradient gel electrophoresis and 16S rRNA sequencing are currently being used successfully in the research setting and may someday be available for use in clinical practice.[7,8] Currently, biofilms cannot be visualized in skin biopsies submitted for routine light microscopy due to collapse of the glycocalyx during the dehydration process9 and require special techniques for visualization of the intact biofilm structure such as electron, epifluorescence, or confocal laser scanning microscopy (CLSM). Conventional therapy is characteristically ineffective against biofilms, as the minimum inhibitory concentration (MIC) of antimicrobial agents has been shown to be 10 to 1000 fold greater than for planktonic organisms.[10] Antimicrobial resistance can be attributed to the EPS serving as a physical barrier to antibiotic penetration, plasmid exchange facilitated by close proximity between organisms, and the low metabolic activity and growth rate observed within biofilms.[4,6,11] In addition, decreased susceptibility to antimicrobial agents may also be related to an increased frequency of mutations, which result in upregulation of efflux pumps and antibiotic degrading enzymes such as betalactamase.[12]
Biofilms present a unique challenge to today's clinician and evidence for their involvement throughout dermatology is constantly unfolding. Herein, we will present current knowledge regarding the role of biofilms in cutaneous disease along with potential therapeutic strategies for the management of biofilmassociated infections.
Wounds
In the United States, approximately 6.5 million patients are affected by chronic wounds[13] and their treatment significantly impacts the health care system with an estimated $25 billion spent annually.[14,15] Chronic wounds present an optimal environment for microbial proliferation and while the association between infection and delayed wound closure has long been established, little is known regarding the mechanisms by which bacteria inhibit healing. In a clinical study of 66 wounds of various etiologies, 60% of chronic wounds were shown to contain biofilms as compared to 6% of acute wounds, indicating the possible role of biofilms in wound chronicity.[16] This study also demonstrated the presence of multiple species within the chronic wound environment existing in the form of highly organized biofilms. Traditional cultures identified Staphylococcus, Pseudomonas, and Enterococcus as the predominant organisms, while molecular analysis additionally revealed the presence of strictly anaerobic species.[16] In fact, a recent profiling study utilizing 16S RNA sequencing in 15 chronic wounds demonstrated an average of 17 genera in each wound, with the majority being anaerobic bacteria.[17] These polymicrobial communities have long been underappreciated due to the shortcomings of standard culture techniques, yet they have important clinical implications as interspecies interactions are likely operative in promoting biofilm pathogenicity.[17] Biofilms have a negative effect on wound healing as evidenced by their ability to induce keratinocyte apoptosis in vitro[18] and inhibit re-epithelialization in an in vivo animal wound model.[19] In addition, biofilms may also augment the inflammatory response characteristic of chronic wounds, thus promoting tissue damage and further contributing to the nonhealing phenotype.[20] It has been suggested that a biofilm-based wound care regimen would incorporate a multifaceted approach with debridement as its most essential component.[6] In addition to removing devitalized tissue that serves as a fertile environment for bacteria, debridement physically disrupts the biofilm structure, resulting in a period of reassembly during which organisms are increasingly susceptible to antimicrobial therapies.[21] Novel antibiofilm agents that have been proposed for use in chronic wounds include lactoferrin, which inhibits bacterial adhesion and has been shown to decrease biofilm mass,[4] as well as xylitol, which disrupts glycocalyx formation.[7] When used in combination, these agents exhibit a synergistic effect and, in vitro, have been shown to decrease the viability of a dual species Staphylococcus aureus (S. aureus) and Pseudomonas aeruginosa biofilm when added to a silver dressing.[22] Future anti-biofilm therapies may also target quorum sensing, as promising results were shown in a murine wound model, where RNAIII inhibiting peptide, a specific staphylococcal quorum sensing inhibitor, resulted in deficient biofilm formation and improved the rate of healing.[19]
Atopic Dermatitis
Atopic dermatitis (AD) affects 10–20% of children with 60% of cases occurring within a child's first year and 85% before the age of 5.[23] Although spontaneous resolution is seen in a majority of patients by 18 years of age, many cases persist into adulthood as evidenced by the 1–3% prevalence of AD among the adult population.[24] It is well known that AD patients are colonized with S. aureus and this organism has been shown to exist in both dry skin as well as areas of severe dermatitis.[25] Disease severity has been directly correlated to the degree of S. aureus colonization and therapy generally fails to improve symptoms in the presence of high S. aureus counts.[26] CLSM has demonstrated the presence of biofilms on mouse skin inoculated with AD S. aureus isolates,[27] as well as in skin stripping and biopsy specimens from 11 AD patients.[9] The difficulty in eradicating S. aureus colonization with conventional antibiotic therapy may be due to the presence of biofilms. It is hypothesized that normal skin microflora, such as Staphylococcus epidermidis (S. epidermidis), has an important role in suppressing the growth of S. aureus by metabolizing sebum and, thus, creating a low pH environment that is inhibitory to pathogenic organisms.[28] Since S. aureus and S. epidermidis exhibit similar antibiotic susceptibility, a logical rationale for therapy may be to specifically target S. aureus biofilm. A recent in vitro study[29] examined the effects of farnesol and xylitol on S. aureus biofilms and showed that each agent alone inhibited a different stage of biofilm formation and, when used concomitantly, they inhibited biofilm formation and also disrupted mature biofilm. The MIC of farnesol was lower for S. aureus than S. epidermidis, indicating the potential of this agent to selectively target the pathogenic organism. In a clinical study of 17 patients with AD,[28] a 0.02% farnesol and 5% xylitol (FX) combination emollient cream significantly decreased the number of S. aureus organisms, as well as the ratio of S. aureus to total aerobic skin microflora with an observed increase in coagulase-negative staphylococci. S. aureus biofilm, demonstrated in the intercellular spaces of the stratum corneum prior to therapy, was completely absent after 7 days of FX topical application. No adverse effects of FX were noted after 4 weeks of therapy. Ideal topical agents for the treatment of AD should selectively reduce pathogenic biofilm and restore the balance of skin microflora without the irritant effects typically seen with current topical germicides.[29]
Acne
Acne affects approximately 45 million individuals in the United States with most patients aged 12–24 years old, where the prevalence has been shown to be as high a s 85%.[30] Evidence for the presence of biofilms in acne is predominantly derived from the ability of Propionibacterium acnes (P. acnes) to form biofilms both in vitro and on implanted medical devices. In addition, sequencing of the P. acnes genome reveals the presence of genes involved in the production of EPS and QS molecules.[31] P. acnes strains isolated from acne patients form biofilms in vitro that are characterized by increased lipase activity as compared to planktonic organisms.[32] This may explain a pathogenic role for P. acnes biofilms in acne, as lipase is not only a well known virulence factor, but it also produces irritant fatty acids that promote inflammation[33] and enhance P. acnes adhesion to the sebaceous follicle.[34] Keratin plugging has long been considered a key component of acne pathogenesis, and the adhesive properties of the EPS produced by P. acnes biofilms in sebum may be responsible for the tenacious binding of keratinocytes to the infundibular epithelium.[35] The observed clinical trend towards decreased efficacy of topical antibiotics may be explained by their usage over time or by the presence of biofilms, as biofilm-associated P. acnes exhibits increased resistance to commonly used anti-acne agents.[36] In addition, the extended length of treatment necessary for acne to respond to oral antibiotics further suggests that biofilms are a key pathogenic factor in this condition.[37] An in vitro study[32] evaluating multiple anti-acne agents alone or in combination found that only 0.1% triclosan, 5% benzoyl peroxide + 0.5% erythromycin, and 5% benzoyl peroxide + 1% clindamycin were effective in both reducing biofilm mass and killing >99% of biofilm-associated P. acnes. Interestingly, 5% benzoyl peroxide alone was ineffective unless combined with erythromycin or clindamycin, possibly as a result of antibiotics inhibiting protein synthesis and, therefore, making P. acnes cells vulnerable to benzoyl peroxide generated radicals. It should be noted that although 30mM azelaic acid was bactericidal, it did not reduce biofilm mass. Minocycline was the only agent in its class that removed biofilm and displayed the greatest bactericidal effect of all the tetracyclines tested. It has been postulated that the success of isotretinoin therapy may be related to reduction of sebaceous gland size with a subsequent decrease in sebum production, thus depleting the nutrient source for P. acnes biofilm.[35] The effectiveness of photodynamic therapy may also be due to an indirect effect on biofilms mediated by decreased sebaceous gland activity.[38] Future acne therapies may incorporate specific biofilm production antagonists or agents that alter the physical and biochemical properties of the pilosebaceous unit in order to create an unfavorable environment for P. acnes biofilm.[39]
Candidiasis
Candida albicans (C. albicans) is a dimorphic yeast that typically exists in a commensal state on mucocutaneous surfaces.[40] In the setting of predisposing factors such as immunosuppression, systemic antibiotic therapy, endocrinopathies, excessive moisture, or ill-fitting dentures, this organism becomes an opportunistic pathogen causing local infections of the skin, nails, and mucous membranes, and in some cases disseminated systemic disease.[41] Recent in vivo animal models demonstrate the ability of C. albicans to form biofilms on mucosal surfaces suggesting that biofilm formation and its characteristic tissue adherence play a key role in promoting Candida infections in these sites.[42] Although it has been suggested that C. albicans forms mucosal biofilms when there are changes in host immunity or alterations in the mucosal ecology or integrity, it is unknown if this organism always exists as a biofilm, even in its commensal state.[43] Cutaneous Candida infections such as intertrigo and onychomycosis may also involve biofilm-associated organisms, although this has not been studied. Oropharyngeal candidiasis (OPC) is seen in 5% of newborns, 10% of the elderly, and is the most common opportunistic infection in AIDS, affecting 90% of these patients.[42] Acute pseudomembranous candidiasis, or thrush, is a common clinical presentation with its characteristic white plaques presumably due to biofilm formation.[44] In a murine OPC model, BCR1, the master transcription factor for Candida biofilms, was shown to be involved in attachment to host cells, promoting epithelial invasion, and protecting C. albicans from neutrophilic attack.[45] C. albicans biofilms have also been shown to overexpress the cell wall polysaccharide, β-glucan, which may be involved in regulating the host immune response and promoting antifungal resistance.[44] Chronic atrophic candidiasis, also known as denture stomatitis, is seen in up to 70% of denture wearers and is caused by ill-fitting dentures compromising what is normally an effective mucosal barrier.[46] Denture stomatitis can be directly linked to biofilm formation as dentures are abiotic surfaces that have been demonstrated to harbor C. albicans biofilms.[47] Angular cheilitis is commonly seen in patients with denture stomatitis, suggesting that biofilms may also play a role in this type of infection. While routine and uncomplicated candidiasis typically responds to treatment with traditional antifungals such as the azoles, the ineffectiveness of these agents in recurrent and persistent Candida infections is thought to result from the presence of biofilms. Most of the information regarding Candida biofilm drug resistance stems from in vitro studies, yet these findings are likely applicable to the clinical setting, as in vitro and in vivo C. albicans biofilms have similar architectural structure, growth kinetics, and genetic determinants.[42] Candida biofilms exhibit a 30 to 2000 fold increase in resistance to amphotericin B, fluconazole, itraconazole, and ketoconazole as compared to planktonic organisms.[48] Subpopulations of cells that exhibit extremely high levels of antifungal resistance[49] as well as the drug penetration barrier function of the EPS[50] have been demonstrated in C. albicans biofilms. Recently developed antifungal agents such as the echinocandins and liposomal formulations of amphotericin B have been shown to be effective against C. albicans biofilms,[51] but are currently available only for intravenous administration. Gentian violet has shown efficacy on in vitro isolates from OPC lesions and may act by inhibiting germination and forming radicals, which enhance penetration through the biofilm matrix.[52] Additional therapeutic strategies that may hold promise for the treatment of Candida biofilm infections include quorum sensing inhibitors, vaccines, anti-candidal antibodies, cytokine therapy, and specific inhibitors of BCR1 and its target genes.[53]
Fillers
Adverse reactions to fillers were previously thought to be due to allergic or foreign body reactions, yet it is now recognized that painful inflammatory nodules in this setting should be considered to be infectious in etiology and immediately treated with antibiotic therapy.[54] Biofilms are possibly the causative factor as evidenced by the persistent nature of filler reactions, difficulty in culturing organisms with routine measures, and the reported high incidence of biofilm-infected medical implants. This has been corroborated by visualization of bacterial aggregates with surrounding eDNA within the filler gel and intervening dermis in biopsies of 8 patients with reactions to polyacrylamide gel.[55] Seven of these patients had been treated with intralesional or systemic steroids, suggesting that reactions to polyacrylamide fillers be treated with antibiotics and that steroids should be avoided. The choice of antibiotic agents as well as the length and mode of administration should be selected based on the filler type and the onset, severity, and duration of infection. Incision and drainage for fluctuant lesions is recommended. Additionally, performing biopsy and cultures is essential for late onset reactions or when particulate fillers are used, keeping in mind that routine cultures are often negative in the case of biofilms.[54] Finally, the performance of filler injections with aseptic precautions is crucial and antibiotic prophylaxis should be considered when injecting into highly colonized areas or acne affected skin.
Other Dermatologic Diseases
S. aureus biofilms have been demonstrated in specimens of bullous impetigo and pemphigus foliaceus[9] while biofilms containing both S. aureus and Streptococcus pyogenes have been identified in non-bullous impetigo.[56] The effects of acetic acid (AA) and hydrochloric acid on S. aureus biofilm formation were evaluated in bullous impetigo and pemphigus foliaceus isolates and were both shown to decrease glycocalyx production.[9] AA had a superior effect in reducing biofilm-associated S. aureus counts, indicating a specific effect of AA unrelated to low pH. In the clinical setting, AA 2.5% ointment was reported to reduce S. aureus counts in pemphigus foliaceus lesions, although no supporting data was presented.[9]
Biofilm formation has also been demonstrated in a murine model inoculated with S. aureus isolated from a furuncle.[57] Treatment with a combination of imipenem and roxithromycin showed significantly reduced S. aureus counts in lesional skin, while treatment with either agent alone showed no effect.
Biofilms have been implicated in miliaria by a clinical study in which only EPS producing S. epidermidis was capable of inducing lesions after inoculation and occlusion.[58] Biopsy specimens revealed sweat glands blocked with EPS material, further supporting a pathogenic role for biofilms in this condition.
Evidence is lacking to support the presence of biofilms in onychomycosis. Nevertheless, several factors including firm adherence of dermatophytes to the nail plate, presence of dormant fungal elements, ability of yeast to form biofilms, and difficulty of eradication all suggest that biofilms may be operative in this condition.[59]
Conclusion
Biofilms are known to be ubiquitous in nature and modern medical technology continues to unveil their role in an evergrowing number of disease processes. In the field of dermatology, biofilms appear to be taking center stage, and their presence likely explains the chronic nature of many cutaneous disorders. It is expected that further knowledge regarding the molecular mechanisms that govern biofilm formation, their virulence, and drug resistance will vastly improve the limited therapeutic options currently available to today's clinician.
Skin Therapy
Letter.
![]() 喜欢
喜欢
0
![]() 赠金笔
赠金笔