 加载中…
加载中…2014年09月18日
ICD-10 AND ICD-9: WHAT’S THE DIFFERENCE?
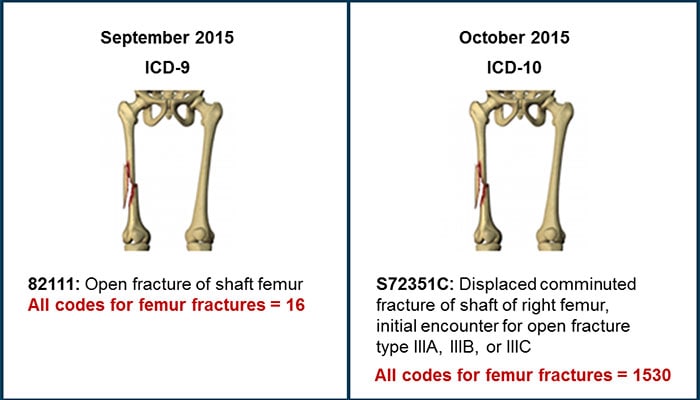
ICD-10-CM diagnosis codes differ from ICD-9-CM diagnosis codes in several ways. The ICD-10-CM code set has been expanded from ICD-9-CM’s 3 to 5 positions (alpha "E" and "V" on the first character) to 3 to 7 positions (alphanumeric character in all positions) and includes placeholder characters ("x"). Other noteworthy changes in ICD-10-CM compared with ICD-9-CM include extensive severity parameters and the reporting of laterality; additionally, many of the new codes cover a combination of diagnoses and symptoms so that fewer codes are needed to describe a condition (Figure).
http://img.medscape.com/article/830/147/830147-figure1.jpg
{kind=link}
Figure.
BUSINESS IMPACTS
ICD-10 implementation will affect both the business of a health care practice and the way clinical practice is managed.
Effects on Systems and Coding
The change to ICD-10 will have an impact on electronic health records (EHRs) and billing systems, and the staff who use them. Because of this, it is important to ask about, review, and understand the relevant software vendors’ plans for updating systems to be ICD-10 compliant.
Although not mandatory, training of staff is recommended to ensure that those individuals who use these systems are well versed in ICD-10 coding. When providing training and analyzing how ICD-10 will affect your practice, focus on the diagnoses most commonly seen in your practice. Typically a few diagnosis codes will account for most of a practice’s business. Zeroing in on these specific codes will help you to streamline your ICD-10 transition.
The change from ICD-9 to ICD-10 will also require a review of forms, such as the superbill or charge master, to determine which ones will require conversion to ICD-10 codes. Software is available to assist with mapping, and CMS offers General Equivalence Mapping. In general, however, providers should not use crosswalking to determine the code for any specific patient condition. Crosswalking may result in selection of an ICD-10 code that roughly matches up with an ICD-9 code, but may not accurately represent the patient’s real condition. According to coding principles, providers should code natively in ICD-10. This means that they should identify and select the ICD-10 code that most accurately represents the patient’s condition based on the official ICD-10 guidelines. Since coding involves clinical analysis, providers should code accurately and according to the guidelines, rather than depending on code crosswalks or equivalence mapping.
Effects on Contracts
Practices should review their contracts to determine any impact of ICD-10. Contracts with payers or other organizations may create other requirements for reporting. Providers should work with payers to ensure that their contracts are compliant with ICD-10 requirements and reflect any operational requirements.
Quality Reporting
Practices should evaluate the impact of ICD-10 on national, state, and regional reporting requirements. ICD-10 codes can be used to report clinical quality measures (CQMs) through EHRs and, because they allow greater specificity, reporting them improves the description of medical data in clinical practices.
ICD-10 codes will also be used as part of the CMS Physician Quality Reporting System (PQRS). Quality reporting gives providers the opportunity to assess the quality of care they are providing to their patients. By reporting PQRS measures, providers also can quantify how often they are meeting a particular quality metric.
The Benefits of ICD-10: Granularity
ICD-10-CM is much more clinically relevant than ICD-9-CM. It better reflects details that describe clinical severity and complexity. The code choices are much less ambiguous than what we experience with ICD-9 today. Because of the greater detail in ICD-10, we can better represent medical necessity of services. Physicians and other providers can help to validate their evaluation and management codes because of the specificity in the new diagnosis codes. And ICD-10 codes permit the documentation to be translated into a much more accurate and clear clinical picture.
The switch to ICD-10 does not affect CPT coding for outpatient procedures. Like ICD-9 procedure codes, ICD-10 PCS codes are for hospital inpatient procedures only.
Clinical Documentation
The structure and granularity of ICD-10 codes will affect clinical documentation, which is necessary for billing accuracy, quality measures, population management, risk management, health care analytics, and patient care.
It is important to remember that inadequate documentation may result in less accurate coding, which, in turn, may cause claims to be denied or may prevent them from being processed in a timely manner. It is recommended that practices review their current documentation against ICD-10 for their most frequent diagnoses. If current documentation will not adequately support ICD-10 coding, practices should consider how to increase specificity to ensure proper coding.
Good patient data require the clinician to observe all facts relevant to patient condition, and to document all of the key medical concepts relevant to current and future patient care. The medical concepts related to ICD-10 are not new to clinical practice. In general, all of the concepts required by ICD-10 are concepts that should be standard for good patient care.
Beyond its clinical value, good documentation is a good business practice, and ICD-10 allows better documentation of patient complexity and level of care.
![]() 喜欢
喜欢
0
![]() 赠金笔
赠金笔